
What is MRI? 🧲¶
Magnetic Resonance Imaging (MRI) is a non-invasive medical imaging technique that uses strong magnetic fields and radio waves to generate detailed body images. Unlike CT scans or X-ray, MRI does not use ionizing radiation, making it safer for repeated examinations.
MRI works by precisely aligning hydrogen atoms in the body using a powerful magnet (typically 1.5T or 3T). When radio frequency pulses are applied and then stopped, these atoms emit signals as they realign. These signals are then processed to generate high-resolution images, which are especially effective for examining soft tissues like the brain, liver and pancreas.
Because of its excellent contrast resolution, MRI is widely used to evaluate tumors, organ structure, blood vessels, and tissue composition. In pancreatic cancer, MRI plays a key role in identifying subtle lesions, assessing ductal anatomy, and detecting metastases.
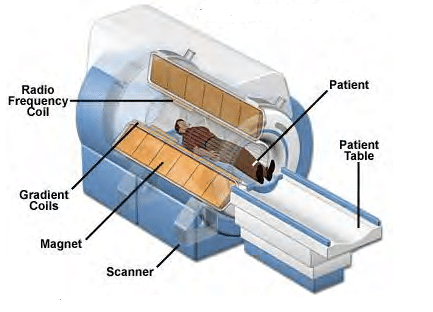

Figure 1: MRI scanners
What is an MR-linac?☢️¶
An MR-linac is a hybrid system that combines a magnetic resonance imaging scanner with a linear accelerator (linac) to deliver real-time image-guided radiotherapy. The goal is to enable precise radiation delivery while continuously visualizing the tumor and surrounding anatomy.
One widely used system is the Elekta Unity, which integrates a 1.5 Tesla MRI with a high precision radiation delivery unit.

Figure 2: MR-Linac system
MRI in Pancreatic Cancer¶
Diagnostic MRI¶
In pancreatic cancer evaluation, MRI serves as a secondary imaging method. While contrast-enhanced CT remains the primary diagnostic tool, MRI is typically used when CT results are unclear or require additional detailed investigation. MRI's primary advantage is its superior soft-tissue contrast and ability to combine multiple imaging sequences in one examination. A standard pancreatic MRI protocol includes:
- T1-weighted in- and out-of-phase imaging to assess tissue composition
- T2-weighted sequences with and without fat suppression to identify cystic lesions and edema
- Diffusion-weighted imaging (DWI) to detect areas of restricted diffusion indicative of malignancy
- Dynamic T1 contrast-enhanced imaging to capture tumor enhancement patterns and assess vascular involvement
- MR cholangiopancreatography (MRCP) to visualize pancreatic and biliary ducts
Pancreatic tumors typically appear as:
- Hypointense on precontrast T1-weighted images
- Variable intensity on T2 images
- Hypoenhanced in the pancreatic phase after contrast injection
- Showing restricted diffusion on DWI sequences
MR-linac MRI¶
Patients with locally advanced pancreatic cancer (LAPC) who are not surgical candidates are often referred for MR-guided radiotherapy on the MR-linac. In these cases, the MR-linac allows for high precision radiation with daily adaptation, which is essential given the pancreas’ proximity to radiosensitive structures like the bowel and stomach.
While the Elekta Unity operates at a 1.5T field strength, similar to many diagnostic MRI systems, it cannot perform the full range of advanced sequences used in diagnostic imaging. Instead, it supports a limited but clinically useful set:
- T1-weighted
- T2-weighted
- Balanced T1/T2
- Inversion Recovery (IR)-weighted
- Diffusion-weighted imaging (DWI)
Visibility in MR-linac images is generally lower due to this reduced sequence set, the absence of contrast-enhanced imaging, lower spatial resolution, and the need for fast acquisitions to minimize treatment time. As a result, small lesions or subtle anatomical details are often harder to detect compared to diagnostic MRI.
Patient Workflow in MR-linac Treatment

|
|